Urticaria (hives/nettle rash)
Urticaria is also known as hives or nettle rash. This condition consists of very itchy wheals that appear on the skin, similar to those that occur after contact with stinging nettles. Swelling (angioedema) may also occur, especially on the face, lips, eyelids, hands or feet.

Table of contents:
Self-Test: Do I have urticaria?
With just a few questions, you can check whether your symptoms indicate urticaria. The test shows which form may be behind it.
Causes
In urticaria, mast cells become activated and release histamine, which leads to itching, wheals and swelling. This common skin condition can occur at any age and may have many different triggers. However, a clear cause is often not found.
- Possible triggers include:
- Infections (e.g. of the respiratory or gastrointestinal tract)
- Allergies (e.g. to foods, insect stings or medications)
- Medications (e.g. pain relievers, antibiotics)
- Physical stimuli such as cold, heat, pressure, light or sweating
- Psychological strain (stress) or hormonal changes
-
Autoimmune processes (the immune system mistakenly attacks the body's own proteins)
Types
Urticaria can occur in two main forms: acute or chronic. Chronic urticaria is further divided into spontaneous and inducible forms.
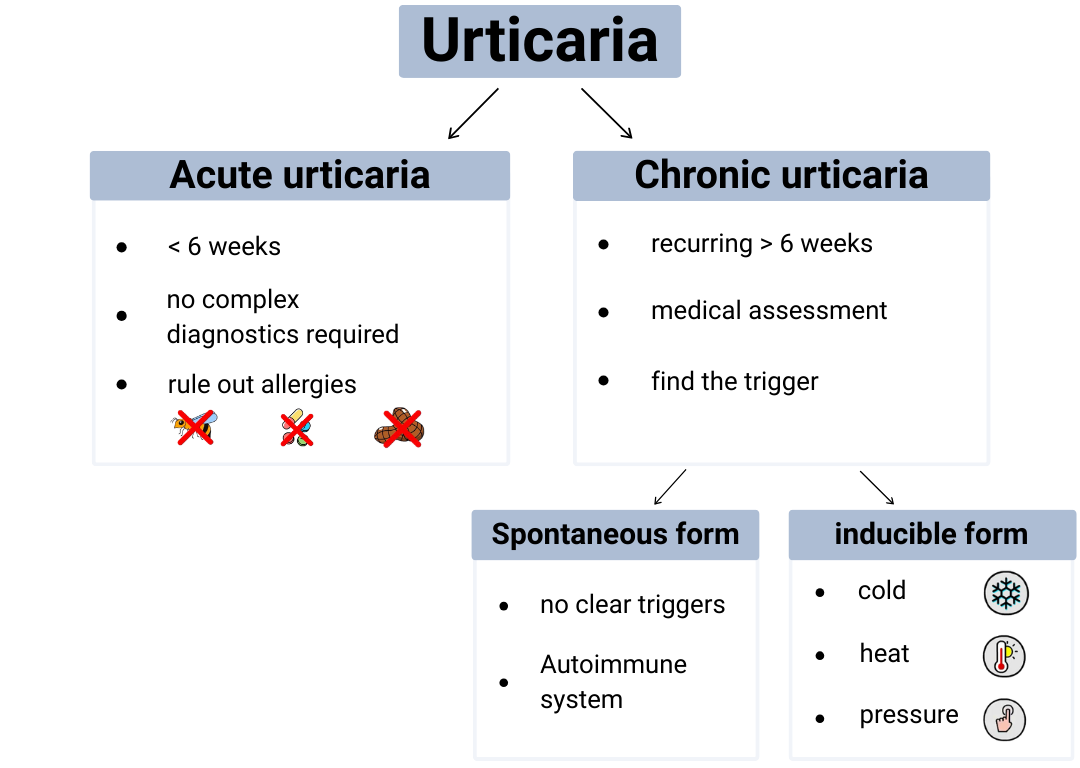
In acute urticaria, the condition appears in episodes that may occur once or repeatedly. The wheals are usually temporary and often disappear within minutes or hours. In this form, episodes usually stop after six weeks, meaning that extensive diagnostic testing is generally not necessary.
However, if acute urticaria occurs after a wasp or bee sting, after taking medication, or after certain foods, an allergic reaction should also be considered. In such cases, careful evaluation is important to rule out a potentially dangerous allergy.
Chronic urticaria tends to last longer and reappear repeatedly. A consultation with a specialist in allergology or dermatology is recommended in order to identify possible triggers and initiate effective treatment. The spontaneous form occurs without a clear trigger. Autoimmune processes are suspected to play a role – meaning that a malfunction of the immune system activates mast cells. The inducible form, on the other hand, occurs only in response to specific stimuli such as cold, heat or pressure on the skin.
Common forms:
After vigorous rubbing, scratching or pressure from tight clothing, line-shaped wheals appear. The skin itches and burns. The wheals usually disappear within one hour.
Wheals or angioedema develop within a few minutes when the skin comes into contact with cold (cold air/wind, liquids or solid objects) and then warms up again. The skin symptoms usually last around one hour. In severe cases, systemic reactions up to anaphylactic shock may occur.
The skin becomes red and wheals appear after physical or sporting activity, but also after passive warming, for example during a warm bath.
- In some people the symptoms are also triggered by:
- emotional stress
- hot or spicy food and drinks
Symptoms usually last between 15 and 60 minutes.
The skin becomes swollen and red when pressure is applied to it. The skin reaction appears 30 minutes to 12 hours after the pressure and may last up to 72 hours.
Itchy and/or burning wheals appear when the skin is exposed to visible light and/or ultraviolet (UV) radiation. Skin changes usually appear within a few minutes.
Symptoms
The main symptoms of urticaria (hives) include:
Wheals are well-defined, superficial swellings of the skin that itch intensely and are surrounded by redness. They appear suddenly and usually disappear within 30 minutes to 24 hours.
Angioedema refers to deeper, larger swellings of the skin or mucous membranes, often affecting:
- the lips
- eyelids
- hands
- feet
- genital area
They may cause a feeling of pressure or tingling and can last up to 72 hours.
In spontaneous urticaria, the entire body is often affected. In the inducible form, usually only the areas exposed to the triggering stimulus are affected.
Diagnosis
In acute urticaria, extensive diagnostic testing is usually not necessary. Further investigations are only required if there is suspicion that urticaria occurred as a symptom of an allergic reaction (for example to foods, medications or insect venom).
In chronic urticaria, evaluation is more complex. Various possible causes and triggers must be considered, while other diseases must also be excluded.
The first step is a detailed discussion with the doctor (medical history). The following circumstances should be documented as precisely as possible:
- use of medication
- physical exertion
- stress
- travel
- timing of symptom onset
Keeping a symptom diary for a period of time can be very helpful.
In chronic spontaneous urticaria, further examinations are usually carried out in order to:
- rule out other diseases with similar symptoms
- identify possible causes and triggers
If medical history and physical examination indicate chronic inducible urticaria, provocation tests with the suspected trigger are performed. Using standard measurement methods, the diagnosis can usually be confirmed and the individual threshold at which symptoms occur can be determined.
Treatment
Urticaria can usually be treated well. Depending on the form, three main approaches are available – individually or combined.
Sometimes it is enough to identify and avoid personal triggers. If you know what causes the skin reaction – for example:
- cold
- heat
- pressure
- stress
- certain medications
you can often prevent or reduce future flare-ups.
Second-generation antihistamines are most commonly prescribed. They can also be taken in higher doses and over longer periods of time. If high-dose antihistamines alone are not sufficient, urticaria can additionally be treated with biologic therapies. These modern medicines are usually antibodies that inhibit specific substances or immune cells in the body and thus reduce excessive immune reactions. In severe flare-ups, systemic corticosteroids may also be used for short periods.
In certain forms of chronic inducible urticaria – such as cold, solar or cholinergic urticaria – repeated exposure to the trigger can lead to temporary tolerance. However, this usually lasts only a few days, meaning the procedure must be repeated regularly (for example daily cold showers in cold urticaria). Since such methods can trigger stronger reactions or circulatory problems, they should only be carried out after medical consultation and, if necessary, under medical supervision.
3 Tips
- Identify and avoid triggers
Write down when and what causes the symptoms – for example cold, heat, pressure, stress, infections or certain medications. This can help identify and avoid possible triggers. - Cooling for itching
Cool compresses or gels can relieve itching. However, avoid extreme cold – especially in cold urticaria. - Wear comfortable clothing
Loose, soft and breathable clothing prevents friction and pressure on the skin. It can also help to increase contact areas, for example with wider bag straps or wider shoulder straps.
Further personalised advice and support are available free of charge via the aha! infoline: aha.ch/infoline
Facts and figures
- Urticaria can occur in all age groups, including infants and young children. Women are slightly more affected than men.
- About one in five people experience at least one episode of urticaria during their lifetime. The chronic form affects approximately 0.5% of the population in Europe.
Frequently asked questions
Urticaria can be triggered by various factors, for example:
- certain infections
- allergies to certain foods or medications
- physical stimuli such as heat or cold
- stress
In many cases, however, no clear cause can be identified.
Cooling compresses or lotions may help relieve itching. Antihistamines are very effective in treating urticaria. If symptoms are severe or recurring, or if an allergy is suspected, medical advice should be sought.
Acute urticaria usually resolves on its own within a few hours or days. If symptoms persist longer than six weeks, the condition is called chronic urticaria, which should be medically evaluated and treated.
No. Urticaria is not contagious. It results from an overreaction of the body’s immune system and cannot be transmitted to other people.
If symptoms occur frequently, last a long time or are very severe, a medical examination is recommended.
- Immediate medical help should be sought if:
- swelling occurs in the face or throat
- breathing difficulties develop
Editors: aha! Swiss Allergy Centre in co-operation with the Scientific Advisory Board and Dr. med. Dr. phil. Anna Gschwend.
Final revision of the website content: 17.03.2026
Thank you for the support
Table of contents:
Free consultation
for affected persons & relatives
Summer break: 20.07.–02.08.



